
Getting diagnosed with Patulous Eustachian Tube can be difficult.
You are your best advocate!
Understanding how PET occurs and the signs and symptoms are crucial for an accurate diagnosis.
Do you have PET?
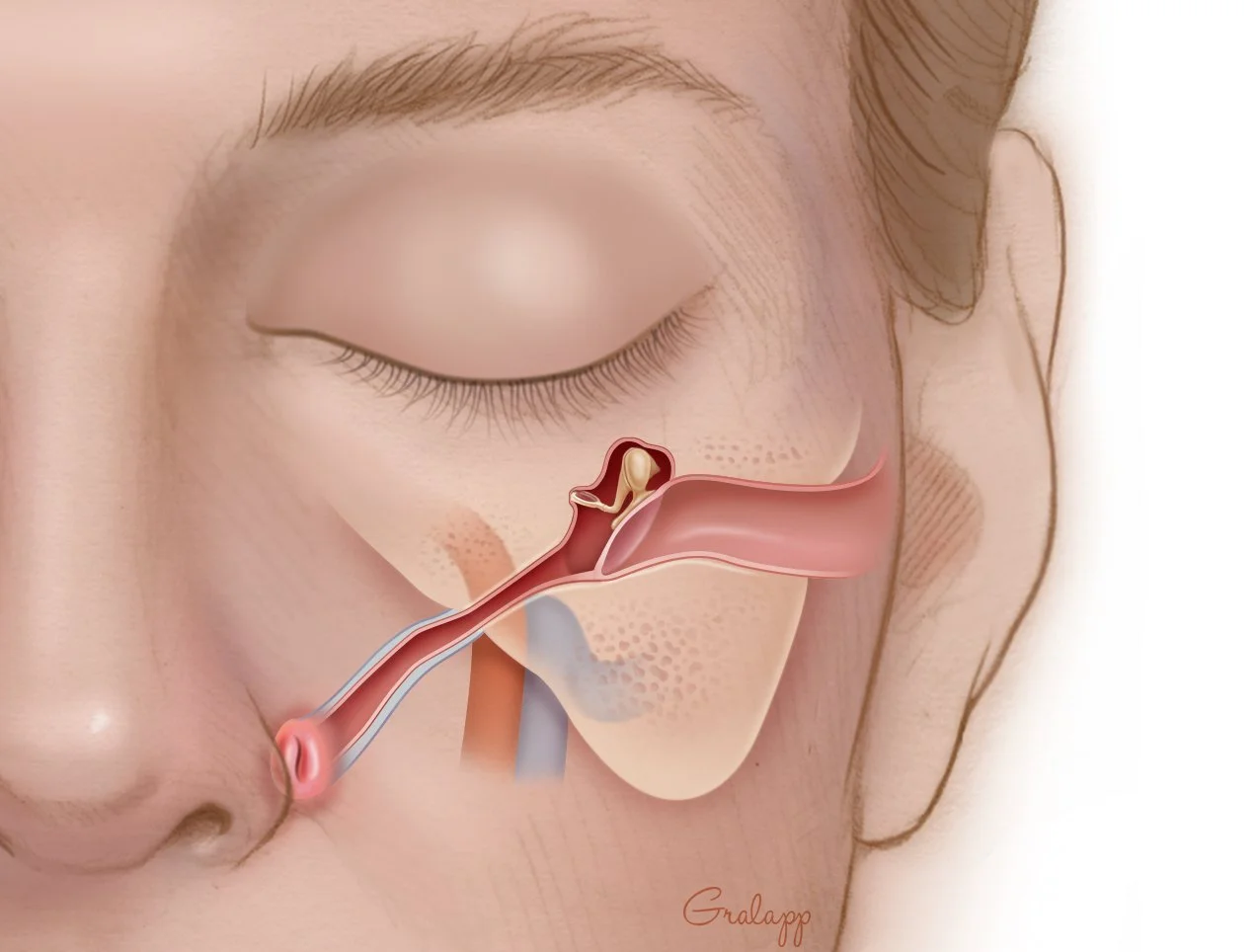
On the right side of the image, the internal structures of the ear are visible, including the ear canal, eardrum (tympanic membrane), and the ossicles (tiny middle-ear bones).
Leading away from the middle ear is the Eustachian tube (auditory tube), which angles downward toward the back of the nasal cavity (the nasopharynx). This tube helps equalize air pressure behind the eardrum.
Physiology of a Patulous Eustachian Tube*
Understanding WHAT is happening to you is vital to being an active participant in your own care
Eustachian Tube (Ear to Nasopharynx)
Entrance to the Eustachian Tube
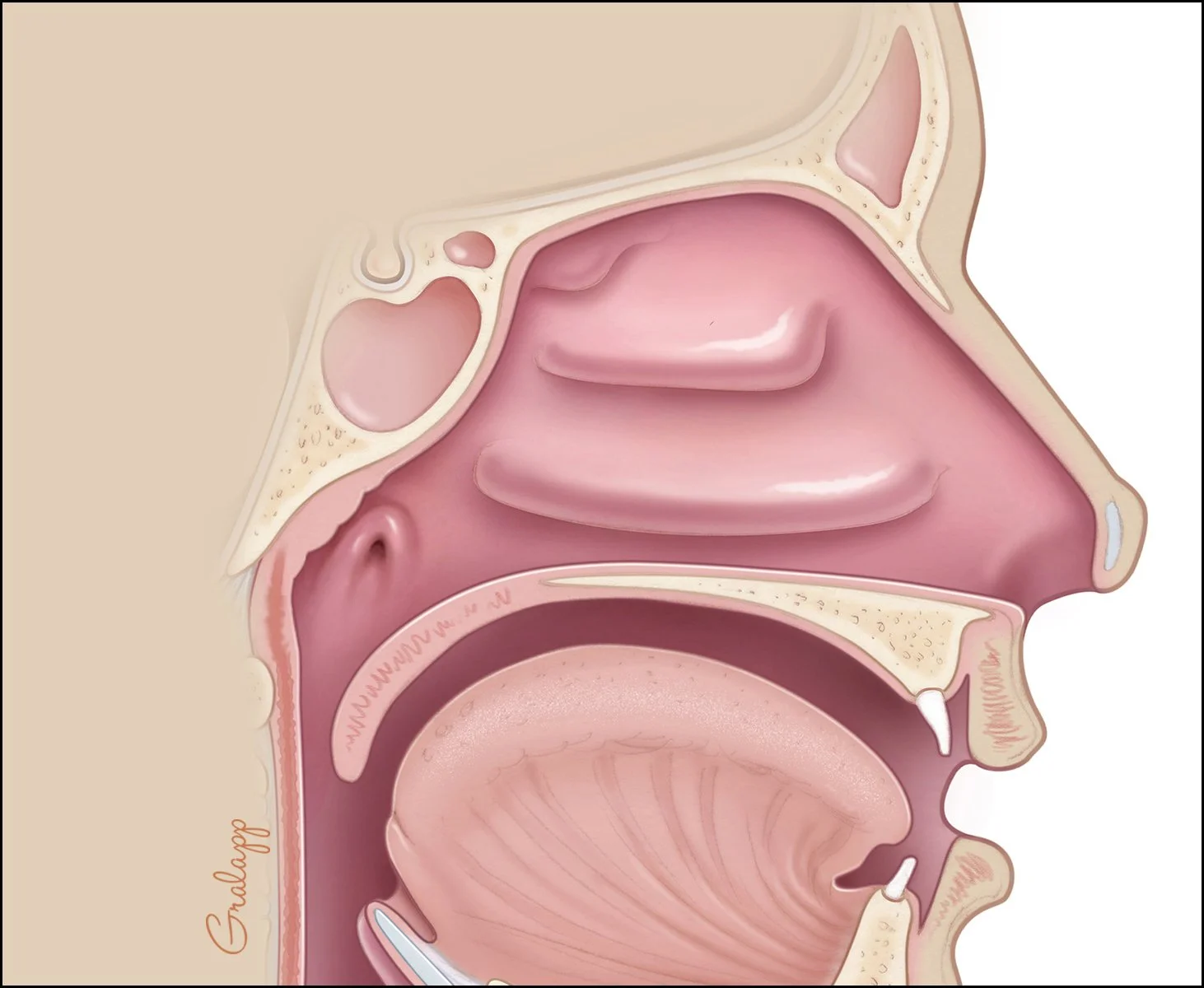
In this anatomical view, the entrance to the Eustachian tube (also known as the auditory tube) is a key feature located in the nasopharynx.
Visual Appearance: The entrance appears as a distinct, vertical, slit-like opening or small oval recess in the side wall of the upper throat.
Location: It is situated directly behind the nasal cavity and the nasal conchae (the bony ridges inside the nose), and just above the level of the soft palate.
Function: While the tube itself is hidden behind the tissue in this view, this opening is the critical point where air enters from the throat to travel up toward the middle ear (as seen in the previous illustration) to equalize pressure.
Opening (ostium) of the Eustachian tube
Functional Context
In a healthy state, this opening remains closed to protect the middle ear from nasal secretions and pressure fluctuations. It only opens momentarily—driven by the TVP and LVP muscles—to equalize air pressure between the middle ear and the atmosphere.
With PET, the opening remains open instead of closed.
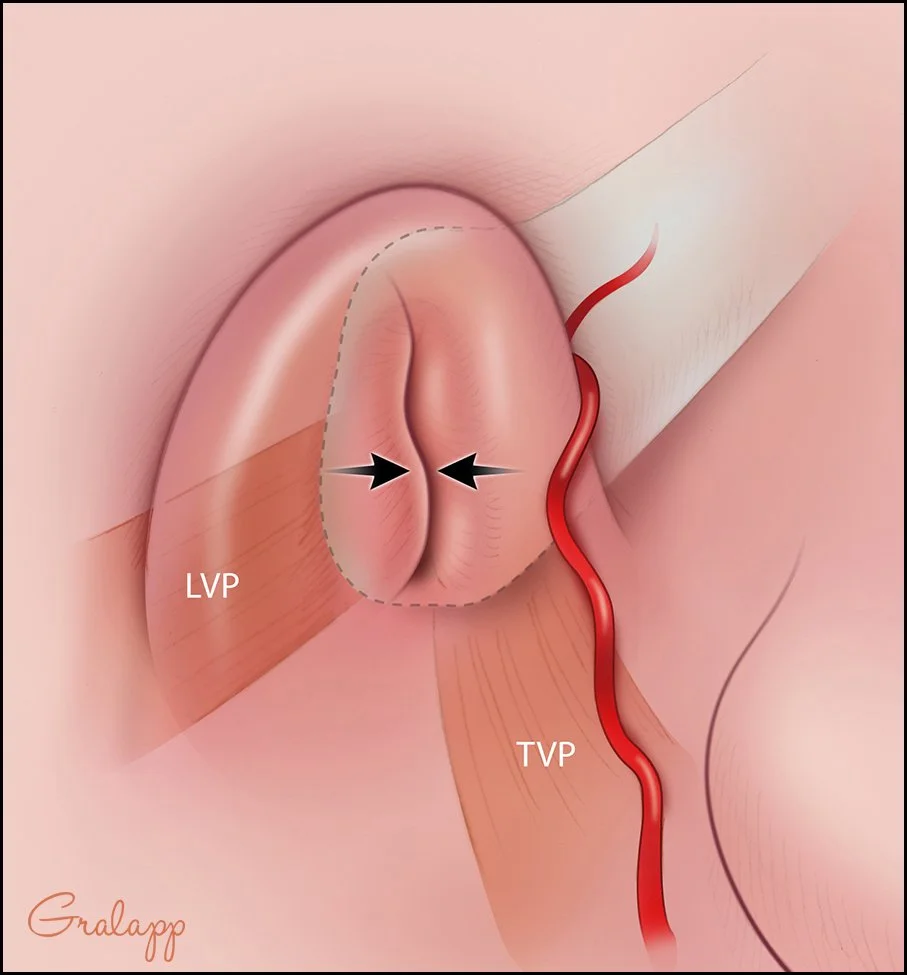
The image highlights the muscles responsible for controlling the opening and closing of the tube:
Ostium (Opening): The central vertical slit, indicated by two black arrows pointing inward, represents the pharyngeal opening of the tube.
LVP (Levator Veli Palatini): This muscle is shown to the left of the opening. It helps elevate the soft palate and contributes to the structural movement around the tube.
TVP (Tensor Veli Palatini): Positioned below and slightly to the right of the opening, this muscle plays a primary role in "tensing" the soft palate and actively pulling the Eustachian tube open during actions like swallowing or yawning
A Patulous Eustachian Tube
Implications of a Patulous Eustachian Tube (PET)
While the image shows a healthy temporary opening, it also serves as a visual representation of what happens in Patulous Eustachian Tube (PET)—a condition where the valve remains chronically "open" or "patulous" instead of staying closed at rest.
This opening allows for sound and breath from your sinus cavity to enter the ear and to cause autophony, one of the hallmark symptoms of PET.
* Images are pulled from https://otosurgeryatlas.stanford.edu/otologic-surgery-atlas/surgical-anatomy-of-the-ear/eustachian-tube/
*Dr. Jackler and Ms. Gralapp retain copyright for all of their original illustrations which appear in this online atlas. We encourage use of our illustrations for educational purposes, but copyright permission should be sought before publication or commercial use.
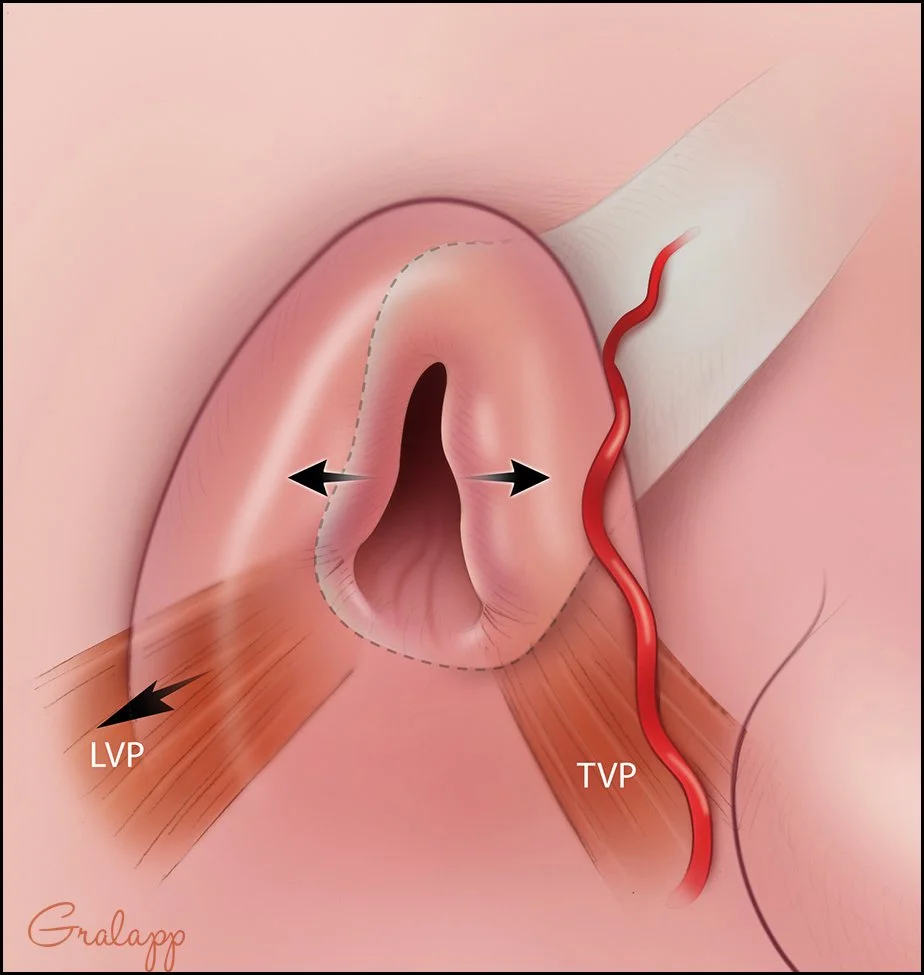
In this "open" state, the following anatomical changes are visible:
Active Dilation: Unlike the closed slit seen in previous views, the opening is now a wide, dark, teardrop-shaped opening.
Muscular Contraction: The black arrows indicate an outward pull. The Tensor Veli Palatini (TVP) and Levator Veli Palatini (LVP) muscles work in tandem to pull the lateral wall of the tube away from the medial wall, momentarily breaking the mucosal seal.
Functional Goal: This opening typically occurs during swallowing, yawning, or sneezing to allow air to pass from the nasopharynx into the middle ear to equalize pressure.
Common symptoms of PET
Autophony: The open ostium creates a direct, unobstructed acoustic bridge between the throat and the middle ear. Patients hear their own voice, breathing, or heartbeat echoing loudly inside their head.
Pressure Fluctuations: Without a closed valve, rapid pressure changes from nasal breathing travel directly to the eardrum. This can cause the eardrum to move in and out (excursion) with every breath.
Aural Fullness: The constant exposure to nasopharyngeal pressure can create a persistent, uncomfortable sensation of "fullness" or "clogging," even though the tube is actually over-ventilated rather than blocked.
What does autophony sound like?
Autophony is the hearing of a “echo” inside your head when you speak. It is also hearing your breathing sounds directly in your ear. It is a symptom that is often difficult to describe to those around you who have never experienced it. Some sufferers equate it to putting a bucket over your head and then talking into the bucket.
Craig Collinson provided all of us with the most accurate way to describe PET to those around you.
Digital otoscope can help identify eardrum moving
Another hallmark sign of PET is an eardrum that moves when pressure is put on it from the nasal side. Air and sound enter the middle ear from the open tube and exert pressure of the ear drum from the inside. Luckily, this is also something that we can observe, and it’s great information to take to your doctor!
Purchase a basic bluetooth enabled otoscope and connect it to your phone. We recommend the Bebird brand of otoscopes (we are not affiliated). These are inexpensive, connect easily with your phone, and you can take pictures and videos to send to your doctor.
See if your drum moved in and out with normal breathing. If it does not, block your nose and blow (LIGHTLY!) in and out and see if your eardrum moves. If it does, make sure you record a video and take it to your doctor.
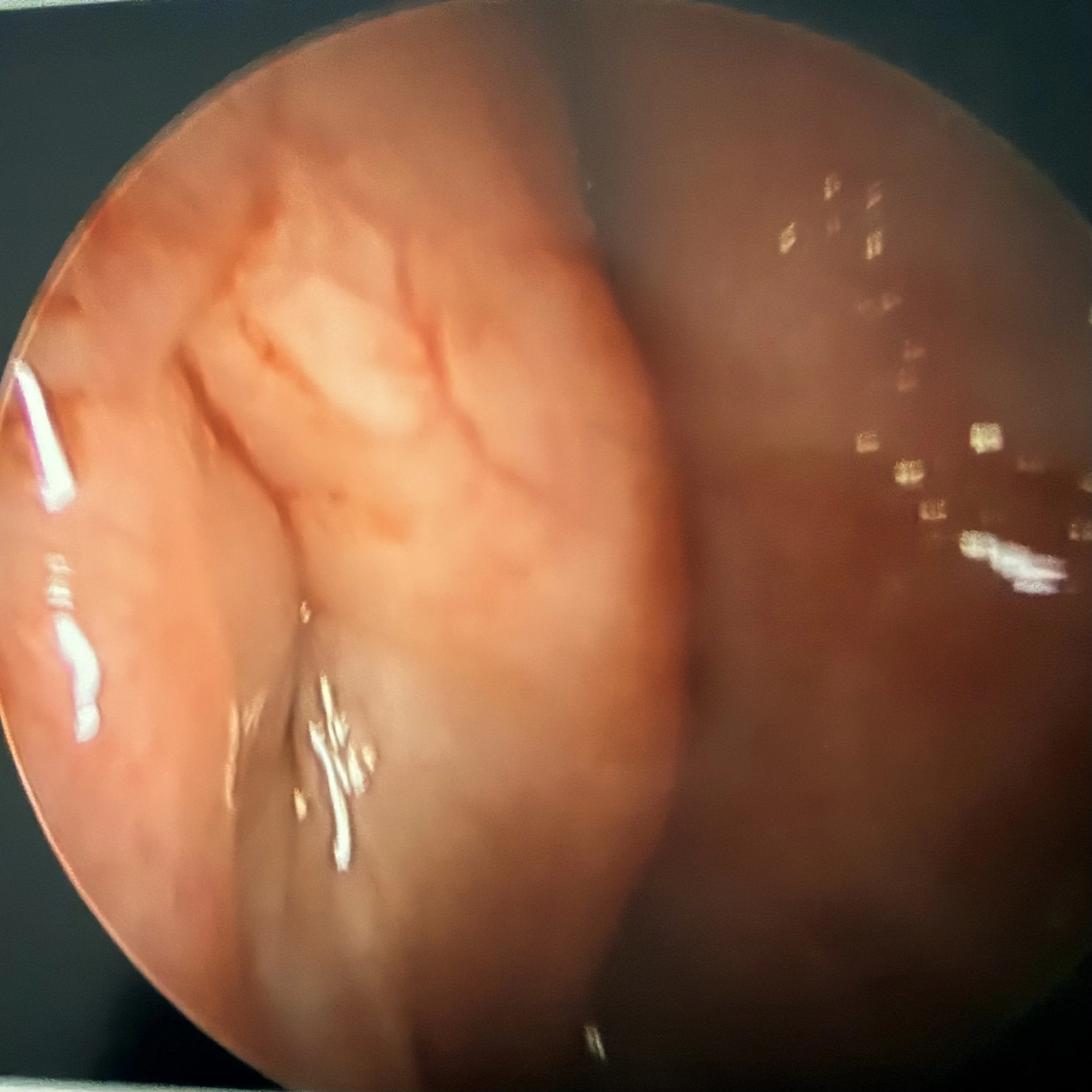
Endoscopic view of eustachian tube opening before and after surgery
Below are before and after images from one of the team members here at CFPET. These images are used for educational purposes only.
Before Surgery

Primary Pathology: The image demonstrates a Patulous Eustachian tube (PET), characterized by an abnormal, persistent patency of the tubal lumen at rest.
Anatomical Characteristics:
Lack of Closure: There is a distinct longitudinal gap or cleft visible, indicating a failure of the normal mucosal closure between the anterior wall and the posterior cartilaginous cushion (torus tubarius).
Patent Lumen: The pharyngeal ostium is visibly open, appearing as a dark, vertical fissure or "keyhole" defect extending into the cartilaginous portion of the Eustachian tube. Normally, this valve should appear as a tightly closed slit when at rest.
This persistent opening of the tubal valve is the classic anatomical presentation of a patulous Eustachian tube, which allows sound and air to travel freely between the nasopharynx and the middle ear cavity, leading to symptoms like autophony.
After Surgery
Primary Result: The image demonstrates successful mucosal coaptation (closure) of the Eustachian tube orifice, indicating the restoration of the anatomical valve seal at rest.
Anatomical Characteristics:
Obliteration of Defect: The previously noted patent lumen or longitudinal cleft is no longer visible. The anterior tubal wall and the posterior cartilaginous cushion (torus tubarius) are now in direct apposition.
Tissue Volume/Augmentation: The mucosa and underlying structures appear fuller or more voluminized compared to a typical patulous state. This increased tissue bulk is consistent with surgical intervention such as an injectable filler or cartilage graft, aimed at plumping the area to close the defect.
In short, this image shows a structurally successful surgical outcome, with the resting "keyhole" defect physically closed.